
Before Doing Anything Else
When you walk into my office, you will see the sign on the wall…. BREATH.
At least once a day, I hear a joke from a patient “Thanks for reminding me, I sometimes forget”.
Although they say it jokingly, many times, they would admit that sometimes, they forget to breathe.
It’s interesting. We can live without food for a month or so, we can live without water for a few days. But how long do you think we can live without breathing?
How could we forget?
Forgetting to breathe or experiencing irregular breathing patterns can be concerning, and it’s important to understand the potential causes and seek appropriate medical attention if needed. Here are some common reasons for irregular breathing or forgetting to breathe:
Stress and Anxiety: Stress and anxiety can lead to shallow breathing or breath-holding. When you’re anxious or stressed, you might unconsciously change your breathing patterns, leading to irregularities.
Panic Attacks: In severe cases of anxiety or panic disorders, individuals may experience panic attacks characterized by rapid, shallow breathing or even hyperventilation. This can sometimes make it feel like you’re forgetting to breathe.
Breathing Disorders: Conditions like sleep apnea can disrupt your breathing during sleep, causing pauses in breathing that you may not be aware of. This can result in daytime fatigue and cognitive issues.
Medications: Certain medications, such as opioids, sedatives, or muscle relaxants, can depress the system and cause irregular breathing patterns.
Medical Conditions: Some medical conditions, like chronic obstructive pulmonary disease (COPD), asthma, or congestive heart failure, can affect your ability to breathe regularly. Neurological disorders may also impact your ability to control breathing consciously.
Physical Activity: During strenuous exercise or physical activity, it’s common for breathing patterns to change. Some people may momentarily hold their breath or breathe irregularly without realizing it.
What is the Diaphragm?
Breathing is a complex process that involves various muscles, with the diaphragm being the primary muscle responsible for initiating inhalation. However, during certain circumstances or when additional respiratory effort is required, accessory muscles may also be recruited to aid in the breathing process.
Diaphragm:
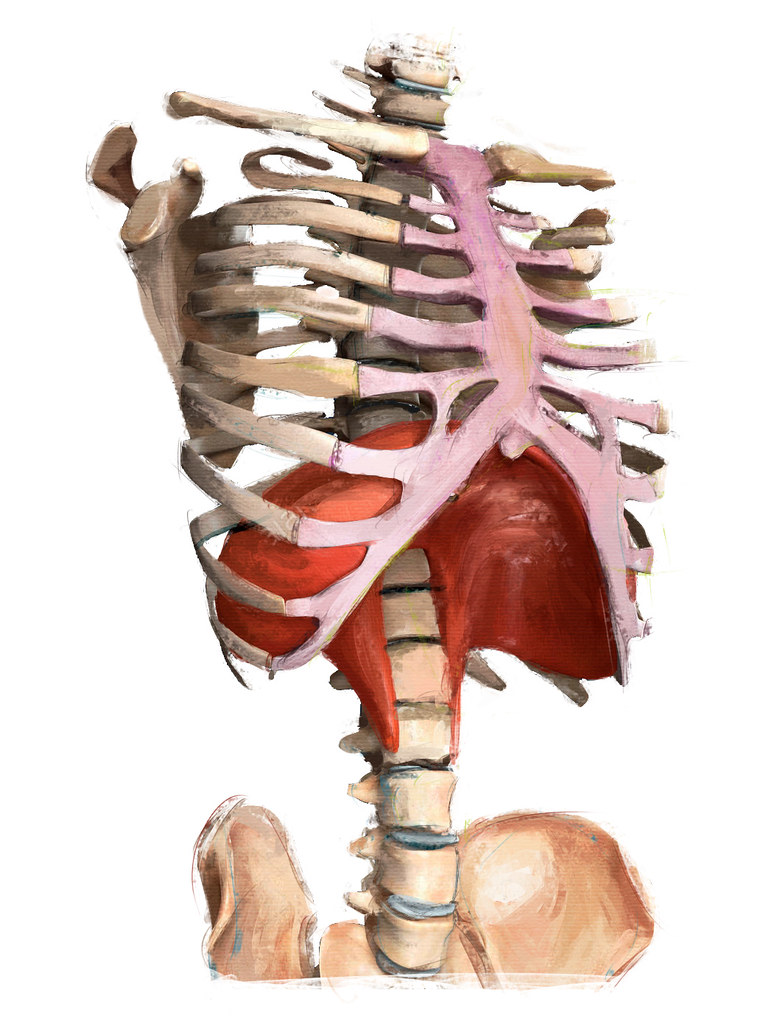
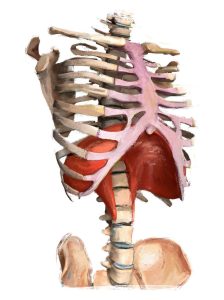 The diaphragm is a dome-shaped muscle that separates the thoracic cavity (containing the lungs and heart) from the abdominal cavity (containing the digestive organs).
The diaphragm is a dome-shaped muscle that separates the thoracic cavity (containing the lungs and heart) from the abdominal cavity (containing the digestive organs).- During normal, quiet breathing, the diaphragm contracts and flattens, which increases the volume of the thoracic cavity, causing a decrease in air pressure inside the lungs. This pressure difference allows air to flow into the lungs.
- The diaphragm is considered the primary muscle of respiration and is active during both inhalation and exhalation. It plays a crucial role in the mechanics of breathing.
Accessory Muscles for Inlation:
While the diaphragm is the primary muscle for inhalation, certain situations may call for additional respiratory effort, leading to the recruitment of accessory muscles.
The main accessory muscles for inhalation include:
- External Intercostal Muscles: These muscles are located between the ribs and assist in lifting the ribcage upward and outward during deep inhalation, increasing thoracic cavity volume.
- Sternocleidomastoid (SCM) Muscles: The SCM muscles, located in the neck, can lift the sternum and clavicles during labored or forced inhalation.
- Scalene Muscles: These muscles, located in the neck, can elevate the upper ribs and further assist in deep inhalation when needed.
- Trapezius and Pectoralis Major Muscles: These shoulder and chest muscles can help lift the ribcage and expand the chest when extra effort is required.
Accessory Muscles for Exhalation:
Normally, exhalation at rest is a passive process, driven by the relaxation of the diaphragm and other muscles involved in inhalation.
However, during forced or active exhalation, certain muscles come into play, including the internal intercostal muscles and the abdominal muscles (rectus abdominis, external obliques, and internal obliques). These muscles help compress the ribcage and abdominal contents, increasing pressure in the thoracic cavity to expel air more forcefully.
The recruitment of accessory muscles for breathing typically occurs during situations that demand increased ventilation, such as physical exertion, respiratory distress, or certain medical conditions. In healthy individuals, normal breathing primarily relies on the diaphragm. However, in cases of respiratory diseases or conditions, the use of accessory muscles for breathing can become more prominent, and this may be a sign of respiratory distress that requires medical attention.
What happens when we don’t optimally use the diaphragm?
1. The diaphragm is designed to be used ALL the time. It’s what keeps us alive. The accessory muscles are only to be used when necessary. Often, when we start using the accessory muscles instead of optimally with the diaphragm, we start to develop things symptoms of neck pain and shoulder pain. As well, because those muscles get tired quicker, we also experience more fatigue when having to use those muscles. Imagine, lifting a bowling ball all day long, your muscles would get tired, right? Same as these muscles, they were not designed to be used all day long.
2. The diaphragm ends where the hip flexors begin. As such a diaphragm that doesn’t move properly will often impede the hip flexors and create hip-like pain as well as low back pain.
3. The esophagus pierces the diaphragm to go into the stomach. A hiatal hernia forms when the sphncter between the esophagus and the stomach is above the diaphragm and then can’t close properly. Even if it’s not a full hiatal hernia, tightness here will cause indigestion, heartburn and reflux.
4. The heart blood, but the diaphragm along with other horizontal structures helps with flow of the lymphatic system and drainage. A tight diaphragm will cause issues with drainage.
5. The diaphragm is optimally placed, above the digestive organs, stomach and liver. The good movement of the diaphragm helps to pump the organs so that they function well.
Ways to Improve the Movement of the Diaphragm
Given where the diaphragm is located, making sure the thoracic spine, ribs and chest is moving well will indeed help the diaphragm move better.
With Pilates, we focus a lot on improving posture. Naturally, with better positioning of the spine in general, breathing definitley improves.
In fact, in a 2014 research in the Journal of Physical Therapy, Pilates helped improve breathing, chest expansion, and lung function in COPD patients.
What You Can Do Now…
Try this. Close your eyes. Take a moment and observe your breathing. Are you feeling the belly expand and relax? Or the movement is more in the upper chest and shoulders?
Observe how easy it is to breath in and breath out. Is it shallow? Is it rapid?
Now sit on your sit bones and straighten up. With a breath in, rotate to the right. As you exhale, come back to the center. Then next breath in, rotate to the left. And exhale, back to center. Repeat this 5 times in each direction.
Then go back to observing. Has your breathing changed? Feeling it more in your belly? Do things seem easier? Lighter?
If you sit all day in front of a computer, do this every couple of hours. It might even prevent that post-lunch slump because you’re getting more oxygen into your system!